
 This is the second in our series of articles designed to assist radiologists with the transition to ICD-10-CM, which will be used in place of ICD-9-CM for reporting diagnoses to Medicare beginning on October 1, 2015. Our goal is to help you fine-tune your documentation to assure the best coding and uninterrupted reimbursement under ICD-10. Our first article covered Documentation for Pain and we also previously posted other information to help radiology practices prepare for this major change. A large number of diagnostic imaging exams deal with the assessment of fractures and the documentation of these exams will require some pieces of information that were not always included in radiology reporting until now.
This is the second in our series of articles designed to assist radiologists with the transition to ICD-10-CM, which will be used in place of ICD-9-CM for reporting diagnoses to Medicare beginning on October 1, 2015. Our goal is to help you fine-tune your documentation to assure the best coding and uninterrupted reimbursement under ICD-10. Our first article covered Documentation for Pain and we also previously posted other information to help radiology practices prepare for this major change. A large number of diagnostic imaging exams deal with the assessment of fractures and the documentation of these exams will require some pieces of information that were not always included in radiology reporting until now.
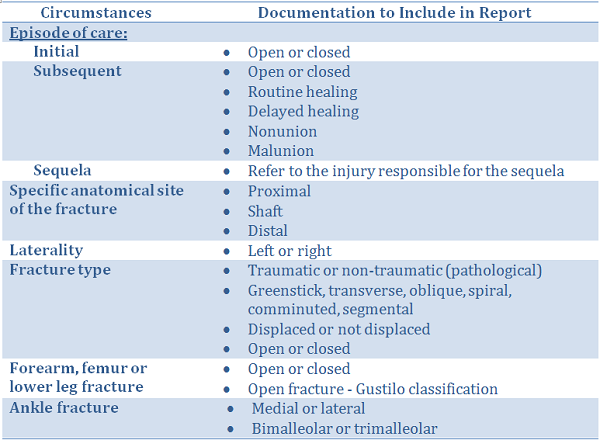
Documentation Requirements for Fracture Assessment
Identification of the Episode of Care is information that was not usually included in most radiology reporting but it now will be essential for the correct coding of fractures or other injuries. Providing this information as a part of the patient history will assist your coders in applying the proper ICD-10 code. Here are the definitions of the three types of encounters:
- Initial refers to encounters while the patient is receiving active treatment for the injury. This will almost always be the case for patients in the Emergency Department.
- Subsequent refers to encounters after the patient has received active treatment of the injury and is receiving routine care for the injury during the healing or recovery phase. This would include a cast change or removal, removal of an external or internal fixation device, a medication adjustment, or other aftercare and follow-up visits following injury treatment.
- Sequela is used for complications or conditions that arise as a direct result of an injury. In these cases the documentation should include reference to the injury responsible for the sequela visit.
When presented with an open fracture, it must be identified as Type I, II or III (plus any applicable sub-categories) using the Gustilo Open Fracture Classification System.
In general, ICD-10 requires more data elements for coding fractures, and all of these should be contained in the body of the radiology report. Coders prefer to have as much information included in the “impression section” of the report as possible. For example, although the laterality of the exam is usually included in the exam ordering description, repeating the right or left side in the impression will enable them to code more efficiently.
Here are some documentation reminders that will allow for proper coding of Fractures under ICD-10:
Practice Workflow Considerations
Clinical information that lets the radiologist know the reason the exam is being ordered is essential to documenting the exam for proper coding. The practice’s information-gathering system should be modified to be sure this information is requested at the time the appointment is made or the exam is scheduled in the ordering system. Any pertinent information not gathered in advance can be obtained by the technologist at the time of the exam, and the revision of tech worksheets can be made to prompt them for these details.
Train your scheduling or insurance authorization staff to get the diagnosis being used by the referring physician whenever possible, and modify their data collection forms to prompt for this information. Referring offices will have their own ICD-10 diagnosis code readily available, and this information will be useful for reference in coding the radiology exam.
Conclusion
The radiologist should always provide the coder with as much specific documentation as possible, with laterality becoming a standard part of the impression section of the report. In the case of examinations to evaluate fractures, including the relevant history will allow proper coding of the episode of care and reference to the Gustilo classification of open fractures will be required. These steps will maximize reimbursement from all payers, even if some of the commercial plans are not ready to accept ICD-10 on October 1st.
Our next topic in this series on ICD-10 issues of specific interest to radiology practices will focus on neoplasms. Be sure to subscribe to this blog to receive the latest in this series of articles to help you maximize reimbursement under ICD-10.
Related articles:
Preparing Your Radiology Practice for the ICD-10 Transition - How to Document Pain

Leave a Reply