 Physicians and other Eligible Clinicians (ECs) who are participating in MIPS under the MACRA rules governing Medicare payments will face requirements that differ depending on whether they are deemed to be “patient-facing” or not. This determination will affect the Advancing Care Information (ACI) and Improvement Activities (IA) components, but not the Quality Performance component of MIPS. In this article, we’ll break-down the key considerations for radiology practices.
Physicians and other Eligible Clinicians (ECs) who are participating in MIPS under the MACRA rules governing Medicare payments will face requirements that differ depending on whether they are deemed to be “patient-facing” or not. This determination will affect the Advancing Care Information (ACI) and Improvement Activities (IA) components, but not the Quality Performance component of MIPS. In this article, we’ll break-down the key considerations for radiology practices.
What is Patient-Facing?
Broadly defined, patient-facing encounters include general office visits, outpatient visits, and certain procedures performed. Medicare has issued a list of CPT codes that are considered to be patient-facing, categorized into three overarching groups:
- Evaluation and Management Codes
- Surgical and Procedural Codes
- Visit Codes
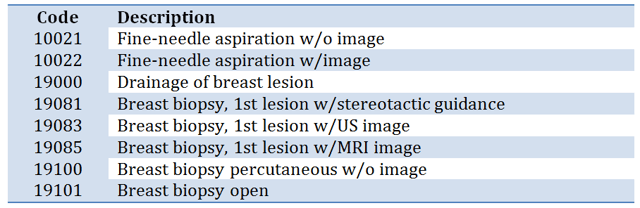
CMS released their list of patient-facing codes for 2017 on December 29, 2016. Of interest to radiologists is the fact that it does not include biopsy or fine-needle aspiration procedures that one might think would be considered patient-facing. These codes were included in CMS prior years’ patient facing codes list but have been removed from the 2017 list for MIPS. For example, the following commonly used codes are not considered to be patient-facing:
An EC will be considered non-patient-facing (NPF) if he or she has 100 or fewer Medicare Part B patient-facing encounters during the annual determination period. The initial determination period is September 2015 to August 2016 for the 2017 reporting period, with a second determination period of September 2016 to August 2017 to identify additional ECs who qualify as NPF. Medicare will automatically determine whether an EC is classified as patient-facing or non-patient facing based on CPT codes submitted; no action on the part of the EC is required. Once an EC has been classified as NPF for a reporting period he or she will continue to be considered NPF for the remainder of that reporting period. In other words, the second determination period cannot cause the removal of the NPF classification.
According to a study undertaken for the Neiman Health Policy Institute, 10% of all radiologists and 9% of diagnostic radiologists would receive the patient facing designation. Thus, we can expect that at least 90% of radiologists will be classified as NPF. The study used 2012 - 2014 Medicare claims data and assumes that billing patterns would not change over ensuing years in a way that would significantly alter the outcome. The report includes the Radiologist Patient Facing Dataset that allows radiologists to look up whether they would have been designated as patient facing in the period of the study.
What Does the NPF Classification Mean?
An EC who is classified as NPF will be exempted from the ACI component of MIPS. The 2017 ACI nominal value of 25% of the MIPS final score will be reallocated to the Quality Reporting category, with the result that Quality will represent 85% of the MIPS final score for 2017.
In addition to the ACI exemption, ECs that are NPF will have a modified reporting requirement in the Clinical Practice Improvement Activities (IA) category of MIPS. In effect, the value of each IA activity is doubled so that high-weighted activities are worth 40 points and medium-weighted activities are worth 20 points. Thus, only 1 high-weighted activity or 2 medium-weighted activities would be necessary to accumulate the 40 points required to maximize the IA component and earn the full 15% towards the MIPS final score.
Group vs. Individual Reporting
Radiology groups that are made up of both patient-facing and NPF ECs will want to look at group reporting. The MIPS rules consider a group to be NPF if 25% or fewer of its ECs are patient-facing. Thus, by reporting as a group rather than as individual ECs, even those ECs who are patient-facing can avoid participating in the ACI component and utilize the lower IA reporting threshold.
Once group reporting is selected for a group practice, participation must occur at the group level across all MIPS categories. Thus, when determining whether to report as a group or as individual ECs, it is important to evaluate which method will allow the practice to optimize its MIPS participation across all of the categories.
Conclusion
Most radiologists are expected to be classified as non-patient-facing (NPF) for the purpose of determining the requirements to maximize their score under MIPS, which will determine the amount of their positive or negative Medicare fee schedule adjustment. Classification as NPF will allow a radiologist to be exempted from the ACI component of MIPS and it will reduce the IA reporting requirements. Groups with some patient-facing radiologists will want to explore group reporting under MIPS.
Healthcare Administrative Partners is committed to helping you understand the changing reimbursement landscape so that you can maximize your radiology practice reimbursement from all payers. Be sure to subscribe to our blog to receive our latest articles in your email inbox as each is published.
Maria Calamaro serves as Product Director for Healthcare Administrative Partners and is the company’s subject matter expert for CMS quality programs. She has over 20 years of experience leading the product development and direction-setting for physician and hospital healthcare applications.
Related articles:
Transitioning Your Radiology Practice to MIPS: The Quality Component Updated
Transitioning Your Radiology Practice to MIPS: Advancing Care Information

